I am deactivating this blog on Jan 23, 2026, just one day prior to my two-year anniversary of my stem-cell birthday in Puebla, Mexico. I just haven’t been posting frequently enough to justify the monthly fee to WordPress, and there are so many other wonderful sources out there related to HSCT, MS, etc to answer questions and exchange thoughts. For any of you who want to keep in touch with me, please send me a WhatsApp at +1 (202) 370-1439, and I can tell you how to find me on social media platforms.
Quick recap of my MS life: I was diagnosed with MS in January 2003, and my MS was fairly gentle for the next 20 years. I attribute much of my good fortune to my strict adherence to the Overcoming MS lifestyle, which I started on Thanksgiving Day 2011. I attribute another good portion of my MS gentleness to pure luck. I took MS drugs directly after diagnosis, as did many people, and their MS was much more aggressive, causing permanent damage and disability within a few years of their diagnoses.
Fast forward to roughly mid-2023, and MS started getting “real” for me. Why then, after 20 good years? As with all things MS-related, there are no clear explanations, but my theory is that it was a confluence of menopause, too many Covid vaccines/boosters, and an unusually stressful work environment.
Life increasingly sucked as my ability to walk deteriorated over a period of roughly six months in a way I had not experienced for the prior 20 years with MS. I had trouble admitting the problem to myself because I had always been able to recover from MS exacerbations by meditating, exercising, vacations, etc.
Starting in roughly August 2023, I tried to avoid any situation that required me to walk in front of others for more than roughly 10 minutes. Crazy! I stopped attending my beloved weight-lifting class at the gym; my muscles were still strong, but my walking was noticeably, temporarily extra wonky after the class. Walking out after class with fellow students could attract the attention of someone who would look at me with concern. I hate “that look.”
I am very energized by social connections, so I initially kept a busy calendar but would arrive before others to restaurants or work meetings so that I only needed to stand to greet people or walk out with the group afterwards. I sat at tables with colleagues or friends until I thought I would die from needing to go to the bathroom because I didn’t want anyone to watch me, walking wonkily from the table to the bathroom or back. As time went on, I delegated work trips to my deputy as professional development for her, but frankly, I was avoiding interactions for fear of someone – a client, heaven forbid – asking what happened to me, or my worst nightmare, reporting to my boss that I was not fit for my job. I often blamed my wonky walking on a bad knee, which was a lie, but an excuse that most people immediately understood and which didn’t generate “that look” or additional questions/concerns/follow-up.
Life was busy, and I couldn’t believe that this problem couldn’t be mitigated by my old trusty practices. By complete accident, I discovered an effective way to ignore my problems. One time when the hot water in an Airbnb stopped working, I took a reeeeeally cold shower out of pure necessity. To my surprise, this “cold exposure” fixed my body for about 40 minutes. After this happy accident, I filled 12 two-liter plastic bottles with tap water at home, and I kept them in my home freezer. Each morning, I filled the bathtub with water and the 12 frozen bottles. During the hour that it took for the bath water to reach the coldest possible temperature — 11C (52F) — I ate breakfast and packed everything needed for my work day. Then, for five and a half minutes, I submerged myself in the ice water up to my shoulders. I emerged with a totally functional body, and I was then “on the clock,” knowing that I had about 40 minutes to be normal.
Normal is so under-rated. For 40 minutes following cold exposure, I walked without thinking about walking. I could look up at the trees, and I didn’t worry about falling. I could walk 10 minutes to my office and spend the balance of my time stopping by colleagues’ offices to wish them a good morning or chat about the day’s challenges ahead, appearing carefree and normal. In that short window of time, I saw the world as a wonderful place and not as a series of dangers and potential humiliations from tripping/falling. But I had a sense of panic, a giant clock ticking as my body slowly returned to its old, wonky MS ways.
Later in my work day, I had just enough energy to walk five minutes from my office to the gym. There, I took another ice-cold shower at the gym, which enabled me to walk and even run a bit on the treadmill…followed by another ice-cold shower to get back to my afternoon at work. I knew this was an unsustainable solution, but cold exposure did allow me to feign normalcy, almost. In between exposures, I would work at my desk, reading email and working like normal desk jockies.
By late 2023, I was taking at least three cold showers or baths each day. More crazy! I didn’t enjoy the cold, but I was addicted to fleeting normalcy. I knew that if I stopped moving, I would have a lot of other health problems.
I literally saw no other options because the MS drugs available were rarely effective for progressive MS. I was angry, confused, and desperate.
Chapter 2 of 6: A Fool To Dream?
Since my 2003 diagnosis of MS, I saw countless news headlines about “ground-breaking” advancements in MS. They were all bullshit for practical purposes. The most recent one at that time was a “quantum leap” in understanding that the MS gene was originally a feature that protected shepherds from diseases of their flocks.
Then I heard a podcast produced by OMS with Dr. Richard Burt of Northwestern University about autologous HSCT (aHSCT): a stem cell transplant that uses your own stem cells taken from your bone marrow to re-boot your immune system. I remember thinking how logical HSCT sounded. I had grown accustomed to hearing of potentially very exciting protocols for treating MS that were in the early stages of research and trial and would not be available for a decade or longer, but HSCT had been done for leukemia and MS for decades by the time I heard the podcast. Why had no doctors ever mentioned HSCT to me as a possibility? More craziness. It all looked very real, but very expensive – over $100,000 in the UK and over $250,000 in the US, after you meet strict qualifications. Clinica Ruiz in Mexico offered HSCT for MS for $57,500. Insurance coverage? I was skeptical.
At age 52, I didn’t look further at HSCT in the relatively cheaper UK, which I heard would not perform HSCT on anyone older than 50. On a whim, I logged onto the website of Clinica Ruiz in Mexico and completed a two-minute HSCT application. Two days later, Clinica Ruiz told me that I was accepted for HSCT. Ha! I immediately suspected them for being a baaaaad place, giving hope to people like me – old and with advancing MS. I told my husband that I had been accepted, but I put aside the possibility of HSCT because it seemed so unreal, far too easy in the MS world where nothing is easy.
Knowing I was accepted for HSCT in Mexico, and that my job contract was coming to an end in Feb 2024, I knew that I had to act fast if I wanted to investigate health-insurance coverage. Because I was employed by a US company outside the US, my health insurance company – Aetna International – was accustomed to covering healthcare outside the US. Within three days, Aetna approved pre-payment of 90% of the $57,500 for HSCT at Clinica Ruiz.
Even the most expensive HSCT on the market is cheaper than life-long MS drugs that cost 10s of thousands of dollars per month in the U.S. The economics of HSCT are undeniably pro-HSCT. Still, insurance companies have historically denied HSCT for MS. In my HSCT group of 19 in January 2024, I was the only person to have insurance coverage. On social media and in my group, there are lots of stories of people doing GoFundMe campaigns, dipping into retirement savings, or selling their homes to afford HSCT. The non-profit HSCT Hope – started by a Chicago lawyer who got a second chance at life thanks to HSCT for MS – started this organization to support people looking for fundraising options/ideas and insurance/medical travel applications and appeals.However, as time goes on, I increasingly hear stories of people’s insurance covering it, too.
Chapter 3 of 6: ¡Viva México!
For nights after Aetna International approved HSCT payment, I couldn’t sleep. I felt at times like a child on Christmas morning, so excited about this possibility. At other times, I was terrified, lost in life logistics of my husband leading the effort by buying air tickets to Mexico, packing, etc. Then I read Everyday Miracles by Dr. Richard Burt, with a foreword by the XIV Dalai Lama, and I never looked back.
After reading this great book, I still had moments of terror, but I felt confident that HSCT was a solid plan to halt progression of my recently aggressive MS. I recalled waves of a similar feeling of fear when I was a child at our public swimming pool. The pool’s rule was that if you started to go up the ladder of the “high dive” diving board, you could not change your mind and descend the ladder. You had to complete your ascent and jump off the terrifyingly high board. The HSCT process was well underway: no going back.
In a nutshell, the 28-day HSCT process in Mexico was among my greatest experiences of my adult life. My husband joined me as my “caregiver,” as required by Clinica Ruiz. From the moment we arrived, the staff at the Center for Outpatient Services (COR) built our confidence, which only grew stronger over the month. They gave us a cell phone that provided precise details for each day’s agenda, as well as pre-programmed texting so that we could ask questions directly to the doctors and nurses, participate remotely in meetings with fellow HSCT patients and caregivers during which the medical team prepared us for each phase of HSCT throughout the month, and connect with my 19 fellow patients and caregivers from the Netherlands, France, Germany, Austria, Sweden, the US, and Canada. Doctors, nurses, and logistics and restaurant staff responded to all questions at all hours of the day or night. Personally, my husband and I never felt more well cared for.
Life at Clinica Ruiz’s residency in Puebla was strangely wonderful. It has a gym for caregivers and patients. Its rooftop deck has an amazing view of one of Puebla’s many volcanoes; nearly each day (except for a few during a phase called neutropenia, following COR health protocols), we spent time on the rooftop with members of our group of 19 fellow patients and their caregivers. The food served three times per day (plus snacks) to me and my husband was tailored to my preferences (as defined by Overcoming MS); others’ dietary preferences were also catered to; the COR restaurant and admin staff were fun and kind for the duration of our stay.
HSCT is a serious medical procedure with chemotherapy etc, but I never felt overwhelmed or in danger because the whole process was so exquisitely managed by HSCT Mexico / Clinica Ruiz. Some of my fellow patients had a rough time with bone pain that they compared to the pain of natural child birth, and nausea, but the medical team was always available to get them through it. I had no bone pain and verrrrry minimal nausea, which was inexplicable but welcome. HSCT for MS does have a history of deaths; however, at the time of this blog, the mortality rate for HSCT for MS is 0.26%, which is lower than hip-replacement surgery.
The most challenging part of HSCT for me was psychology of losing my hair. I chose to buzz-cut my should-length hair before the chemotherapy caused it to fall out in approximately the end of the third week of the four-week process. I have never liked my hair, so I surprised myself by my fear of this moment. In fact, I discovered that I feared losing my hair more than I feared chemotherapy. Surrounded by 19 fellow patients and their caregivers, I felt a camaraderie that helped me dive into the experience and embrace my hair loss as a small price to pay for a chance at halting my MS.
Both my husband and I were really sad to depart Clinica Ruiz.
Chapter 4 of 6: The HSCT Rollercoaster
As I type, I am day +83 following my stem cell birthday on January 24, 2024, when Clinica Ruiz re-injected my stem cells back into my body. Only 10% of HSCT patients experience improvements in symptoms immediately following the procedure. I have felt no distinct improvements yet, so I am not one of those 10%. With the others who are not part of the 10%, I can only wait and see if HSCT halts my MS. The plan is to get an MRI 12 months after HSCT to see if it shows any MS activity. The HSCT rollercoaster – worsening and improvement of symptoms, hope, worry that you are relapsing or a non-responder – can continue for more than a year.
The suspense and isolation of this rollercoaster can be difficult, except for the thousands of HSCT “alumni” around the globe, more than 1,600 of whom got HSCT in Mexico. These alumni are an extraordinarily generous group of people whom I interact with on Facebook* or via the HSCT Warriors podcast. They remind me that my body took years of MS abuse, so it will take time (years) for me to heal, if I am among the people for whom HSCT halts MS. Fingers and toes are crossed.
My baseline during my first 20 years with MS was an EDSS of 0.5 to 1.5. I even ran two marathons. In the year before I discovered HSCT, my symptoms worsened quickly. Clinica Ruiz conducted many tests (blood, heart, lungs, etc etc) just prior to HSCT and my MS was “replapsing-remitting” and a 3-3.5 on the EDSS scale of 10 (10 being worst).
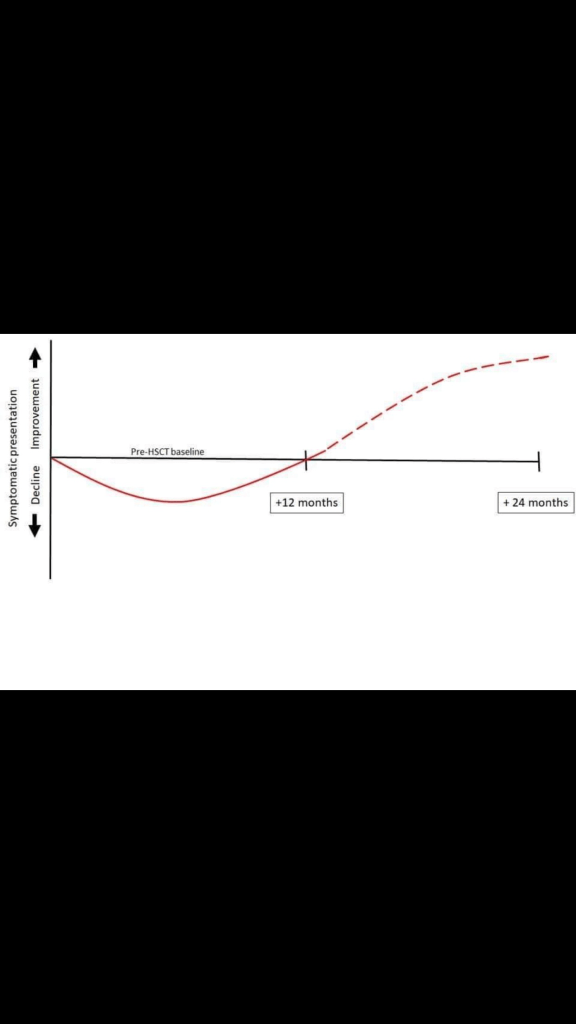
In fact, many people experience a worsening of their symptoms after HSCT during the first year (and even well into their second year) before reaching their pre-HSCT baseline. From there, people’s EDSS scores may or may not improve. I have spoken with several people whose EDSS scores went from 4.5 to 0.5 or similar improvements thanks to HSCT and after more than a decade with MS disability before HSCT.
Actress Selma Blair recorded her HSCT experience at Northwestern University in the movie Introducing Selma Blair, which shows a *much* rougher HSCT procedure than I experienced at Clinica Ruiz, but the movie does not follow her beyond year 1 post-HSCT. The movie implies a level of frustration with her outcome; but her performance in Dancing With The Stars is, in my opinion, miraculous, regardless of her decision to not proceed beyond episode 4.
Many HSCT alumni have public blogs to track their progress during and after HSCT. It is not uncommon for alumni to feel certain that HSCT did not work for them, and then to see improvements 1-3 year(s) after HSCT. Here is one example on Facebook – a 3.5-minute video – where a woman believed in year 2 that she was a non-responder, but in year 3 had reached a point where she could consistently run, paddle, stay out late partying, etc. I spoke to this particular woman in her year 7 post-HSCT, and she was still feeling great. These are stories I have heard repeated over and over by HSCT alumni.
The following graph shows the average experience on the HSCT rollercoaster, recognizing that each body’s recovery rollercoaster is as different as their MS symptoms.
To increase the chances that HSCT will halt my MS, I do just a few fairly simple things. I take two medicines (acyclovir and bactrim), which Clinica Ruiz prescribes to protect you from viruses and other bugs while your new immune system rebuilds for six months following the completion of HSCT. During that time, I must avoid large crowds and wear a surgical mask in public. I follow a “neutropenic diet,” which sounds fancy, but basically means that I eat only cooked food; raw fruits and vegetables are prohibited for six months to mitigate risks of food-borne infections, with the exception of avocados and bananas. Why this exception? Frankly, I don’t know. Six months feels long as I type in month 3, but again, it’s a very small price to pay.
Most people go back to work within a month or two of completing HSCT, while following these precautions. I chose to quit my job mostly because I had saved enough to do so, and I was tired of my career; and stress definitely makes my MS worse. Following HSCT, I started exercising according to the MSing Link protocol, which I have found strategic, structured, and informed by great research. I also walk as much as I can each day, instead of sitting behind my computer for 10+ hours per workday, on weekends, vacations, and holidays, as I did for years in my career.
For what it’s worth, I caught Covid only about three weeks after my stem cell birthday, and it wasn’t bad. I was reeeeeally scared, but Clinica Ruiz monitored me closely and remotely via WhatsApp. I would have gone to the hospital if I had any real concerns. I just took Paracetamol 1 g to keep my fever below 101.5 F. As I type, I also have a bad head cold, which I will hope is a “training course” for my new immune system, as we think of young children getting sick. Many HSCT alumni don’t get sick for more than a year after the procedure. I wish I were one of them, but I won’t lose sleep worrying about my new immune system, which for reasons I will never understand, it working nicely.
Chapter 5 of 6: The Data
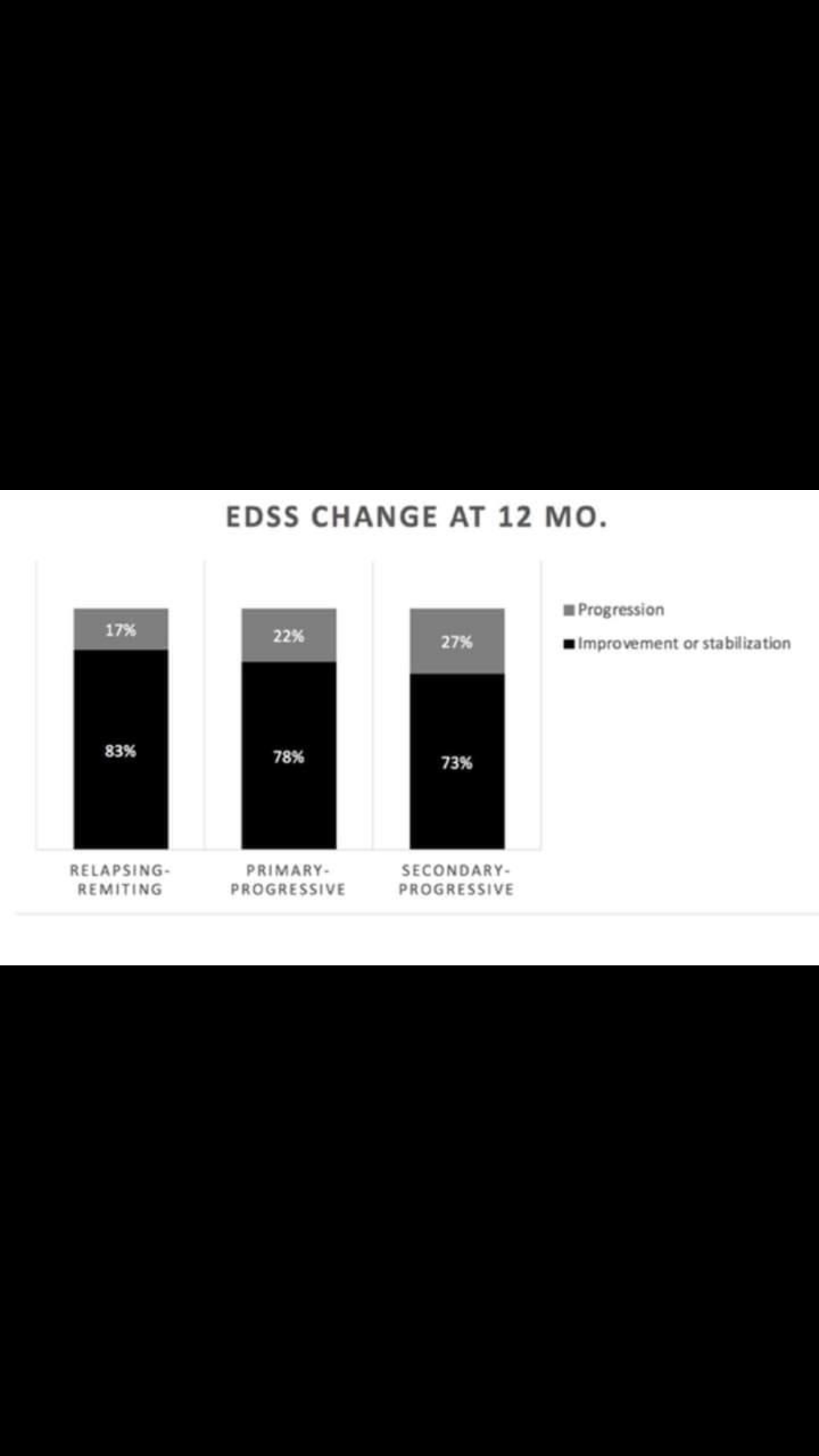
HSCT does not promise to cure MS, nor to improve your EDSS, but it halts progression in a high percentage of recipients (see below), which is better than any MS drug, all of which only promise to slow progression, cost astronomical amounts monthly, and causes really bad side effects in some people. One HSCT alumni put it this way: MS chains you to train tracks. HSCT has a high percentage of a chance to stop the train; MS drugs say they can slow the train. Which would you choose?
HSCT also does not promise to improve your MS symptoms, but so many people experience some improvements in their EDSS. Imagine MS attacking your central nervous system, like a car driving over a road. Over the years, the road can develop potholes, which in MS is permanent damage to the nerves’ protective sheath, called myelin. If HSCT halts your MS, then HSCT removes the car that created the potholes, but it does not fix the potholes. That type of medicine is in the works.
As you can imagine, the sooner after an MS diagnosis that you can get HSCT, the higher your chances of stopping its progression before it even becomes a problem. However, today in the US, you can only qualify for HSCT if you have “failed” three prior MS drugs — if those drugs have failed to halt your MS, which none of them even promise to do. The drugs only “slow the progression.” This requirement to fail three MS drugs is a BS qualification, since these drugs have zero relationship to HSCT, nor to HSCT’s chances of success.
There is a lot of discussion about “flipping the triangle,” which means making HSCT the first action after an MS diagnosis, rather than a last-ditch effort. According to Gavin Giovannoni, PhD, professor of neurology at Barts and the London School of Medicine and Dentistry:
Currently, MS patients are allowed to accumulate a number of disabilities before they can have the most effective treatments, and that is not right…We should be treating MS like stroke, where time is of the essence. And we should be offering newly diagnosed patients the most effective treatments such as monoclonal antibody-based therapies and aHSCT first to prevent too much organ damage.
Chapter 6 of 6: An Unexpected Pathway Leading To Gratitude
Prior to HSCT, many of us alumni preferred to minimize drugs in our lives to the greatest extent possible. Hell, my entire blog site is based on the peer-reviewed, published research that led to my decision in 2014 to stop taking MS drugs. The idea of a natural approach had always been really appealing to many of us. So HSCT – chemo and plenty of other drugs during and for six months after the procedure – was a really unexpected pathway. And, yet, here we are.
Whether or not HSCT works for me, I will continue following the Overcoming MS lifestyle because, as explained in Everyday Miracles, HSCT does not eliminate your entire immune system. Though nobody says that the OMS lifestyle promotes success after HSCT, it is based on more than three decades of research published by Dr. Roy Swank, and it keeps inflammation low. Many HSCT alumni swear by the paleo diet, and I have no desire to convince them to do otherwise. I myself do not want anything to ever spark whatever of MS might remain in me. I enjoy the OMS lifestyle, even if it is not effortless in a context of the Standard American Diet (SAD).
HSCT makes me grateful: (1) for or the opportunity to have gotten HSCT; (2) to Dr. Burt for pioneering HSCT for MS, writing Everyday Miracles for the layman reader and a medical textbook for other doctors who may be interested in performing HSCT for MS, and for speaking to as many MS podcasts as possible to raise awareness; (3) to Dr. Ruiz, lead of the world-class Clinica Ruiz in Mexico, for delivering HSCT for a relatively affordable cost in the most humane and “enjoyable” manner possible and for taking time to personally meet each patient four times during my month-long procedure; and last but definitely not least (4) to all my fellow HSCT warriors globally for their friendship and courage throughout the procedure and the long, loooong rollercoaster.
Footnote:
Facebook HSCT groups: Find the global group by searching for HSCT Hematopoietic Stem Cell Transplant – MS & Autoimmune Diseases, and for Mexico groups, search for Mexico HSCT for MS & Autoimmune diseases.
In late May 2020, as COVID-19 cooled down in Tunisia, which I currently call home, some new friends whom I met just prior to confinement invited me to their home for lunch to celebrate our new freedom. Around the same time, before Tunisia opened its borders to international travel we planned a week-long road trip inside the country with another new friend.
In the lead up to both events, I was so excited. Pretty quickly, however, this excitement was overtaken by a familiar, exhausting discomfort. I am sick of the facade, but I fear what will happen if I drop it and come clean.
I had the honor of being invited to share my story on the podcast “Healing Heroes,” led by Nicolette Richer, PhD and CEO and founder of Green Moustache Cafe (https://www.greenmoustache.com/) based in Whistler, Canada. I met Nicolette at the annual conference of The Physicians Committee for Responsible Medicine in 2018. I have enormous respect for her work. The interview is about 30 minutes and it tells my story of diagnosis until discovery of my role in my health. To listen, clickhere.
My life changed radically for the better when I learned that a mountain of scientific research shows that my daily choices make the difference between wellness and disability in MS. Every day, every bite I eat, every decision I make, I think, “will this keep me healthy?” If ever I am tempted to make a “bad” decision, I ask, “French fries or a wheel chair?” I am motivated. I can easily unplug my temptation. I am empowered. My future is in my own hands.
But what about my past? I cannot help looking back at my life and asking: what did I do to trigger MS? Continue reading “Why Me?”
As I began drafting this story in September 2018, I had a very bad opinion of the U.S. National Multiple Sclerosis Society (NMSS). I know some feel much more positively about it, and that’s not a bad thing. Whatever gives hope to someone with MS, I’m all for it.
The nature of blogs is openness, to a fault at times. Anonymous blogs give writers a license to speak recklessly. Honestly, I want to slam NMSS based on my own perspective, but I value facts, so I decided to reevaluate my opinions.Continue reading “The National MS Society”
Don’t giggle. OK, go ahead and giggle a little. Get it out. Then keep reading. As I researched this topic — medical marijuana for MS — I found that about half of my friends responded with a half-baked smile, while the other half spouted statistics about billions in tax revenues.
Call me a party pooper, but I actually don’t care about getting high or tax revenue, though I hugely appreciate any issue that acts as a lever to legalize marijuana.
I care only about staying mobile and healthy with MS for as long as possible. Forever would be nice. Since I live in the Commonwealth of Virginia, where marijuana is fully illegal as of 2018, I also really care that I could lose my job (and health insurance) if a random drug test finds an illegal substance in my blood, even with a prescription. Even in states where marijuana is legal — for example, California, Colorado, Michigan — legal complications are ugly and serious.
If you read my other blog posts, you know that my wellness strategy for MS is based on a whole-foods, plant-based diet, but I am constantly searching for additional science-based approaches to keep me healthy for as long as possible.
The topic is so complex that I am incapable of explaining most of it succinctly or accurately in my humble little blog. The agenda of the Second National Cannabis Policy Summit in April 2018 brought together representatives of Congress, The Brookings Institution, the Attorney General of DC, doctors, lawyers, civil rights activists, journalists, lobbyists, and others to discuss the most pressing policy challenges and opportunities. For the mildly curious, this 11-card deck provides a nice overview, and for the more curious, this Cannabis 101 series of short videos answers a wide spectrum of questions. Consumer Reports provided a simple set of guidelines on how to shop for CBD.
One aspect that directly impedes my ability to understand how the heck medical marijuana could benefit (or harm) my health with MS is Schedule 1 classification. According to the Controlled Substances Act signed by Richard Nixon in 1970, the federal penalty for trafficking less than 50 kilograms of marijuana, a Schedule 1 drug, is no more than five years in federal prison and up to a $250,000 fine for the first offense. Ouch. Schedule 1 drugs (e.g., heroine, marijuana) are regarded to have no medical value.
One doctor, Mikhail Kogan, who happens to be my primary care physician, is a leader in the campaign to increase research into the efficacy of medical marijuana. As the medical director of The George Washington Center for Integrative Medicine, Dr. Kogan is optimistic but cautious about the powerful compounds in marijuana.
So what about MS? I was surprised at the unequivocal terminology used by a few very reputable sources. Dr. Kogan pointed me to a 2017 report by the National Academy of Sciences, Engineering, and Medicine, described as one of the most comprehensive studies of research published since 1999 on the health effects of recreational and therapeutic cannabis use in a spectrum of illnesses, from cancer to MS to HIV to depression, etc. You can download free chapters (including Chapter 4, Therapeutic Effects, referencing MS) or buy the $65 full report. Conclusions included:
Conclusive or substantial evidence that oral cannabis or cannabinoids are effective for improving patient-reported multiple sclerosis spasticity symptoms (oral cannabinoids); and
Moderate evidence of improving short-term sleep outcomes in individuals with sleep disturbance associated with…[lots of other things and] multiple sclerosis (cannabinoids, primarily nabiximols).
The report highlights the need for a national cannabis research agenda that includes clinical and observational research, health policy and health economics research, and public health and public safety research.
There is also the 2017 article, Cannabis and MS – The Way Forward, published in Frontiers of Neurology of the U.S. National Institutes of Health. The article can be summed up with the following excerpt:
…There are many open questions regarding cannabis use [as an MS therapy], including optimal strains, frequency of use, other dosage questions, risks of long-term use, and which symptoms it effectively treats. These are all important questions in which the NIH and MS foundations should be interested. Unfortunately, up to date, NIH has not funded research grants on the benefits of cannabis in MS (10). Furthermore, there are no current research projects on cannabis funded by the National MS Society (11). Why is this the case? We hypothesize that while grant reviewers make the argument that randomized controlled trials (RCTs) are needed for this research, few if any are possible in the current legal framework…
Nice. Bight me, legal framework. And while I am at it, the U.S. National MS Society can bight me too, since they should be out in front, advocating for sensible legal reform benefiting people with MS. The article also explains the twisted institutional knots and bias that obstruct serious scientific research to answer a long list of questions.
In the margin of this article, several links are provided to other articles on MS and medical marijuana. In the same publication, this 2018 article — Cannabidiol (CBD) to Improve Mobility in People with MS — caught my attention. A quick summary:
…Based on the following considerations, it is our opinion that CBD supplementation maybe advisable for people with MS (PwMS) to reduce fatigue, pain, spasticity, and ultimately improve mobility…It is clear that more research is needed. However, because of the safety of CBD and if the concerns listed above are accounted, we are in the opinion that we already have some good reasons to believe that CBD enriched cannabis is useful to improve the mobility of PwMS.
This article also looks at key considerations, including risk of addiction, contraindications, labeling inaccuracies, and the possibility of testing positive for marijuana.
I am left with a whiff of hope and a mix of disgust and sadness that potential solutions are stuck behind the bureaucratic stupidity of Schedule 1 classification. Regardless of these barriers, the 2017 article mentions that approximately 50% of people with MS already use cannabis, and the 2018 article mentions that 66% of people with MS use cannabis. Time matters for people with MS. Time waiting for reform is time lost to disability. Screw that. No seriously, screw it.
Dr. Kogan prescribed medical marijuana for me in early 2018 in the form of CBDa, one of many, many strains of marijuana, which I take in a tincture (droplet) form in a base of MCT oil to aid absorption. This mix is super tasty. Less tasty, flaxseed oil has the highest Omega-3 content, which is recommended – unrelated in any way to marijuana – by Overcoming MS, but flaxseed oil requires constant refrigeration.
A few questions that I asked when considering whether and how to take CBDa follow:
Dose?Thanks to the scarcity of large-scale studies caused by institutional obstacles, it’s currently impossible to say. In this podcast, Dr. Kogan speaks with Dr. Donald Abrams, one of the world’s leading clinical researchers on medical cannabis and an integrative oncologist at the University of California San Francisco, about the total lack of nomenclature for dosing. In DC, where medical marijuana is legal, Dr. Kogan is not legally able to advise patients on what strain of cannabis to take.
As an impatient patient of MS, I ask: how fricken stupid is that?
Kogan asks, “How do we guide our patients?” Dr. Abrams responds, “That’s the $64,000 question. Go to the dispensaries, tell them what medical condition you have; they deal with other patients who have what you have. See what they recommend.”
Generally, the guidance is to start low and go slow. After more than six months, I take roughly two full droppers (5 mg x 2) of CBDa in the morning and evening.
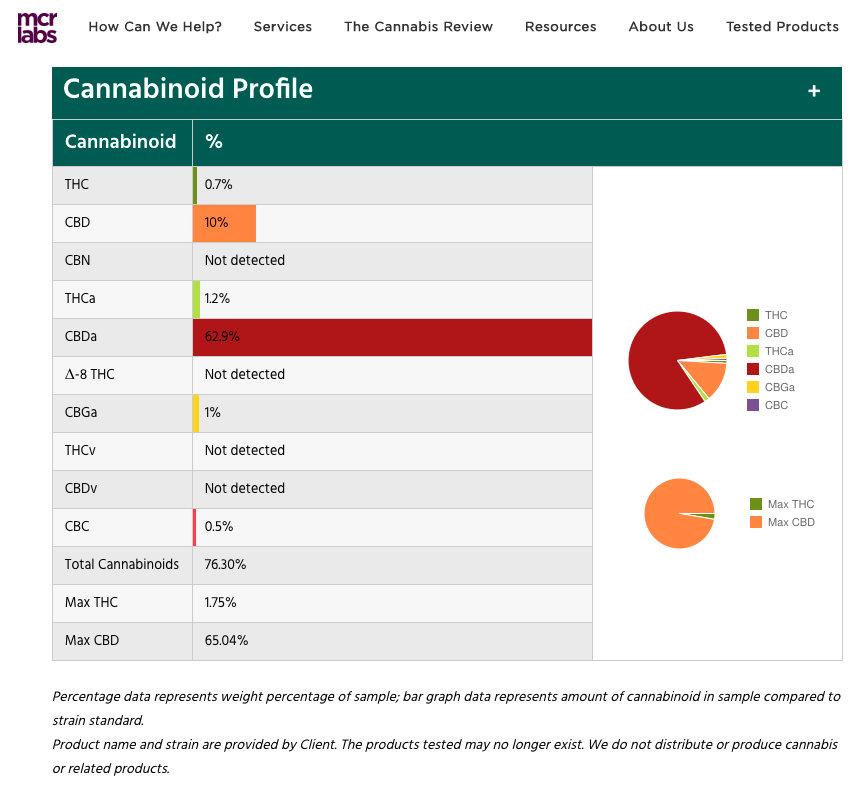
Source?I get my CBDa from a person recommended to me by Dr. Kogan. He has been to this person’s production facilities in Vermont, where the hemp plant is grown organically. The producers than send every batch to MCR Labs in Massachusetts.
Safety? MCR Labs produces a report on the contents of the tinctures that my source produces and sends to me. I provide a screen shot below of the batch sent to me in February 2018. Notice that THC, the psychoactive portion, is at 1.75%. In other words, an illegal substance could show up in my blood test, but the amount would be so low that I could pass the test. However, for whatever crazy reason, it could generate questions/concerns, and so my source told me bluntly, “it is a risk” that my employment could be terminated.
Price?I pay (in 2018) $50 per 300 mg bottle, which lasts roughly a month (or two; my adherence has been imperfect, even with no official guidance on dosing). No, it is not covered by insurance.
Why in tincture form?The veins under our tongues bypass the digestive system, specifically the liver and metabolites, which could mitigate the impact of powerful compounds, and make a bee-line for our brains. Since MS is a disease of the central nervous system, a tincture gets the CBDa to its destination more directly.
How does CBDa make me feel?You know that awesome feeling after you blink? No? Right. That’s how euphoric I feel after taking CBDa. I get no high — zero, zip, nada. That’s what most people seem to want to know. As I said, I do love the flavor. It’s like you have the freshest pine tree under your tongue for a couple minutes. Wow?
So why do I bother with CBDa, given that it ain’t cheap?Several reasons:
First, it is neuro-protective and possibly neuro-generative, so I consider CBDa an additional insurance policy — on top of a meticulously healthy diet, exercise, meditation, and other critical daily routines — for the care and maintenance of my central nervous system, slightly bedraggled after nearly a decade of doing nothing beyond MS drugs after my MS diagnosis in 2003.
Second, medical marijuana has demonstrated clinical benefits and promise in U.S. government-funded studies for MS (linked above) and cancer*, and the FDA approved medical marijuana for pediatric epilepsy**. How can the FDA recognize the therapeutic value, while the definition of a Schedule 1 drug is that there is no medical value? The U.S. government needs to get its ducks in a row.
I am not willing to wait for the political knot to be untangled; I am willing to risk my employment because I can get another job, but I can’t get another nervous system. I feel sorry for anyone whose job is to deny someone access to potential therapies for pain, seizures, immobility, spasticity, etc.
Third, I share with a bit of embarrassment, but in the spirit of truth made easier with an anonymous blog: CBDa seems to have saved me from wicked night sweats, which could result from a spectrum of causes (e.g. peri-menopause, cancer, etc), but which are definitely a symptom of MS rarely discussed in polite company. I had them almost nightly for about a year; now with CBDa, they are an occasional whisper of their former raging strength. That’s the only (but very welcome) physical change I have noticed since starting CBDa, but it makes me wonder what other benefits I could be accruing.
Plant versus pharmaceutical?Dr. Kogan said that there have been so few large-scale studies on medical marijuana that any commercial supplier that says they know the right dose/strain for specific ailments is not being honest.
For me, as long as I have a safe source of medical marijuana, I prefer the basic plant. Beyond my fascination with the science behind the power of a whole-foods, plant-based diet, I learned something mind-blowing: Have you ever heard of your body’s EndoCannabinoid System (ECS)? I had not. Thanks to Wikipedia, I learned that the ECS is a biological system composed of endocannabinoids, which are endogenous lipid-based retrograde neurotransmitters (huh?) that bind to cannabinoid receptors and receptor proteins that are expressed throughout the mammalian central nervous system, including the brain and peripheral nervous system.
What actually is a cannabinoid [kuh–nab–uh-noid]?Simply, it is any of the chemical compounds that are the active principles of marijuana, the dried leaves andandfemaleflowers of the hemp plant (Latin: Cannabis sativa). Cannabinoid = hemp = marijuana = cannabis. It’s far more complicated than that, but my non-scientific brain needs the Dummies version.
So, our bodies have receptors for the cannabinoid compounds in the hemp plant. That factoid brings renewed significance to the power of plants. Wow.
In conclusion, I am not endorsing medical marijuana for you, and I certainly do not feel it is a stand-alone silver bullet. This blog is an attempt to explain why I include it in my large toolbox for wellness. Perhaps someday, reputable research institutions can conduct rigorous, large-scale, double- and triple-blind studies on the bio-mechanics of cannabinoids for MS. Then, if the evidence continues to show efficacy, I hope that insurance companies will make medical marijuana available and affordable to everyone with MS. I can’t imagine how many years that will take, but I am not waiting. Until then, I’ll just enjoy my tasty pine-tree flavored treat.
~~~~~
*Excerpt from link: To summarize, cannabis and cannabinoids are useful in managing symptoms related to cancer and its treatment. Exciting preclinical evidence suggests that cannabinoids are not only effective in the treatment but also in the prevention of chemotherapy-induced peripheral neuropathy. Cannabinoids could be synergistic with opioids in the relief of pain. The safety profile of cannabis is acceptable, with side effects that are generally tolerable and short-lived. Preclinical data suggest that cannabinoids could have direct anti-tumor activity, possibly most impressive in central nervous system malignancies. Clinical data about the effects of cannabis concentrates on cancer are as yet unavailable. Oncologists could find cannabis and cannabinoids to be effective tools in their care of patients living with and beyond cancer.
**Excerpt from link, “…The FDA needed to see solid evidence, meeting rigorous criteria, before approving any cannabis-derived drug for medical therapy. And [this] is the first drug to have achieved these high standards.”
Dr. Caldwell Esselstyn, a barely-retired, 84-year old cardiac surgeon who spent his career at the Cleveland Clinic, said that medicine is “on the cusp of what is truly a seismic revolution.” Dr. Neal Barnard, president of The Physicians Committee for Responsible Medicine, spoke to an audience of a thousand medical doctors, nurse practitioners, and a few people like me — poster children with widely-assumed incurable diseases, treating ourselves with the simplest medicine: nutrition. We were all attending the August 2018 International Conference for Nutrition in Medicine. Dr. Barnard opened by saying that we are on a “wave that hasn’t even begun to crest.” I believe it, if this crowd is any indication of the future.
So many courageous leaders in healthcare spoke at this conference, and not surprisingly, I learned a lot. For example, according to Dr. LaQuandra Nesbitt, director of the District of Columbia Department of Health, there is a greater than 20-year gap in life expectancy between different neighborhoods in Washington, DC. In other words, as she put it, one’s zip code has a greater impact on longevity than one’s genetic code. Here (NYT and food banks) and here (Jack Monroe) are two perspectives that help explain how this could be.
We cannot ethically let this continue, can we?
At lunch, I joined a table of 10 strangers, most of whom were medical doctors in some version of family practice. Listening to them during our short lunch, my opinion of these doctors changed from awe to pity. After all, according to U.S. News and World Report, not one of the top 10 medical schools in the U.S. had an acceptance rate above four percent in 2017. For example, Georgetown University medical school received more than 14,000 applications, but less than three percent of applicants were accepted. My lunch mates were the creme de la creme of achievers in our country and the world. I hardly felt worthy of sitting with them.
And yet, one after another, each doctor described grueling hours and administrative hell in their daily work lives. They were attending the conference for continuing medical education credits, but nothing about the actions of this lunch group — a small sample of the one thousand attendees — were perfunctory. They were all committed to the seismic revolution in health care anticipated by Dr. Esselstyn. Many were volunteering their time and self-funding cooking classes or information sessions after office hours for their patients. At the same time, they were all beaten down by the stress of 15-minute time slots in which to counsel patients about their options for advanced diseases, like diabetes: drugs, diet, or death. Time is up! Good luck!
One 40-year old doctor told me that her employer, a large medical facility, would reduce her annual income if she did not meet specific performance targets. I asked her to explain these targets; I only understood that the targets were administrative gobbledygook — nothing to contribute in any measurable way to her patients’ wellness. She said that she has nearly a million dollars in debt from medical school, was burnt out from the moment she finished medical school, and living with her mother to make ends meet.
We cannot ethically let this continue, either, can we?
Another doctor, Saray Stancic, a keynote speaker at the conference who also has MS, is asking these same questions. Her website explains that her focus is shedding light on the building body of scientific evidence supporting the importance of optimal nutrition and lifestyle in disease prevention. With the help of Kickstarter, she is producing a movie, Code Blue: Redefining the Practice of Medicine, to examine these issues.
As a patient, I have always assumed that doctors could change the tide of medical stupidity, and yet now it seems to me that many doctors are irretrievably stuck. Events like this conference gave us all hope that things will be better. With 86% of our three trillion healthcare system spent on chronic illnesses, we do not have a choice.
I spend much of my free time researching how the U.S. healthcare system can be fixed; day-dreaming about a day when my neurologist will not react angrily when I tell him that I have chosen diet over drugs as my strategy for wellness. According to a March 2018 article in The Hill, “…agricultural subsidies cost taxpayers about $20 billion a year: This includes a massive transfer of wealth from taxpayers to mostly large agribusinesses that are (or should be) fully capable of managing their business operations without this special treatment.” Those subsidies should be directed to health-promoting initiatives, including production of organic fruits and vegetables. Not juices and sugary snacks. Just plain old-fashioned apples, spinach, etc.
The science is so fricken overwhelming for the efficacy and cost savings of nutrition in wellness that I literally get tired of reading the same repetitive, albeit inspiring, medical outcomes. Maybe apples and spinach aren’t sexy enough to catch people’s attention. Hmmm, how can apples and spinach get sexier?
Cue wildly successful Hollywood producer, James Cameron, and muscly 71-year old Arnold Schwarzenegger. Cameron’s next movie due in 2018, The Game Changers, is billed as “a shocking expose of the world’s most dangerous myth: that meat is necessary for protein, strength, and optimal health.” The movie follows elite special forces trainer and winner of The Ultimate Fighter, who traveled the world and “What I discovered was so revolutionary, with such profound implications for performance, health, and the future of the planet itself, that I had to share it with the world.”
I welcome the Hollywood sparkle, while recognizing the *army* of scientists, researchers, and other professionals pumping out mountains of data that said/says the same damn thing, starting decades ago.
I am also learning from unexpected places. Since 2017, my day job is as a project manager on a U.S. federal government contract funded by the United States Agency for International Development, supporting the President’s Emergency Plan for AIDS Relief (PEPFAR). It is the biggest contract ever awarded by USAID: $9.5 billion (yes, that’s a b). Big.
I was initially conflicted about the possibility of working on a project associated with Big Pharma, who royally pissed me off in my little MS corner of the world. My older sister, who has for my entire life never failed to tell me when I am being an idiot (for which I am grateful), became increasingly alarmed as I became more vocal about my mistrust of drug companies. One day after listening for the 100th time to my tirade against drug companies, she finally spoke up, saying “Drugs are not all bad! Childhood leukemia is no longer a deadly disease. The AIDS virus can be suppressed so that patients can live practically normal lives.” I could not argue with her.
From there, I began examining and questioning how my experience fit into the reality. Was I totally wrong? No. Indeed, communicable diseases like AIDS and chronic diseases like MS are fundamentally different. But maybe I could borrow important lessons from AIDS to contribute to a better future for MS and other chronic illnesses. From the United Nations (UNAIDS) website, one can quickly see how clear goals can be a catalyst for action:
By 2020, 90% of all people living with HIV will know their HIV status. (There are currently 36.9 million people living with HIV. Just 75 percent know they are HIV positive. The rest do not.)
By 2020, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy (ART). (Three out of five people are on ARTs.)
By 2020, 90% of all people receiving ARTs will have viral suppression. (Only 47% in 2018 have undetectable levels of HIV.)
When asked if AIDS is a chronic illness or a deadly disease, Warren (Buck) Buckingham III, responded that it depends on where you live. Hmmm, sounds like the words of Dr. Nesbitt regarding your zip code and gentic code for longevity.
By contrast, approximately 133 million Americans, representing more than 40% of the total population of this country have a chronic illness, according to the National Health Council, and that number is projected to grow to an estimated 157 million, with 81 million having multiple conditions. What will it take to wake up the beast of the American consumer?
So I accepted the assignment on the $9.5 billion AIDS project. To give it my best effort to prepare to join this team, I read two books recommended by a woman team leader, who works on this giant project and whose dedication to overcoming the AIDS epidemic mirrors my own passion for overcoming MS: And The Band Played On (by Randy Shiltz) and My Own Country: A Doctor’s Story (by Abraham Verghese). From MS, I understand the profit motive in illness, but I never fully understood the politics of illness until I read these books. You must read them to believe them.
In a nutshell, the U.S. government stalled far too long – decades – before it paid serious attention and dedicated sufficient resources to the AIDS epidemic. Many millions of people died horrible deaths, waiting for projects like this one.
Like AIDS in its early days, chronic illness today is not being taken seriously by the U.S. government. It was the same story with cigarette smoking, when doctors promoted it. As of July 2018, only 26 of 50 U.S. states have enacted statewide bans on smoking in all enclosed workplaces, including all bars and restaurants. Wake up, please.
Unlike AIDS, chronic illness is not as much of a mystery as drug companies would have us believe. In the 1980s, AIDS sparked an international race to identify the virus and develop drugs to suppress it. For chronic illness today, we already know a lot about the root cause of and how to prevent and reverse heart disease, diabetes, cancer, even some cases of MS, and so many other chronic illnesses. We also know that current agricultural and food policies, school lunch programs, subsidy programs, etc. establish perverse incentives and promote more chronic illness.
What we need is courageous public officials to regulate and legislate wellness into our food and education systems. I dream of a gigantic federally funded program — or even a coordinated national government initiative — to address the crippling problem of chronic illness in this country. In the meantime, there are a growing number of private groups, like The Physicians Committee for Responsible Medicine, The T. Colin Campbell Center for Nutrition Studies, etc etc etc; the list is long — churning out huge amounts of research so that, I believe, someday during my lifetime, we will look at today’s U.S. healthcare system as we now look at smoking. And we will ask: what took our government so long to wake up?
Four out of five. Eighty percent of my family has been diagnosed with a chronic illness. I am crazed by my failure to convince them and everyone else I love to adopt my way of thinking about the connection between diet and disease.
What am I doing wrong?
I realize that it is insanity for me to try to change anyone. Since 2011 (seven years at this point) since I changed overnight from a junk-food junky to a whole-foods, plant-based eater, it’s still hard enough to ignore that voice in my head that really wants junk food.
But how can I just sit quietly and watch it happen? According to An Empirical Study of Chronic Disease in the United States*:
“More than two thirds of all deaths are caused by one or more of these five chronic diseases: heart disease, cancer, stroke, chronic obstructive pulmonary disease, and diabetes. Additional statistics are quite stark: chronic diseases are responsible for seven out of 10 deaths in the U.S., killing more than 1.7 million Americans each year; and more than 75% of the $2 trillion spent on public and private healthcare in 2005 went toward chronic diseases…What makes treating chronic conditions (and efforts to manage population health) particularly challenging is that chronic conditions often do not exist in isolation. In fact, today one in four U.S. adults have two or more chronic conditions, while more than half of older adults have three or more chronic conditions.”
MS is not even on the list, though I am among 400,000 people in the U.S. (2.5 million worldwide) with this chronic disease. Officially, nobody dies of MS. Right. MS can just make you feel sidelined from life. Which is, I guess, better than dead.
I believe that all chronic diseases are the same wolf in different sheep’s clothing. That wolf’s name is inflammation, which initiates and promotes diseases of a wide variety. Each person’s genes define how that inflammation manifests itself. The scientific evidence is so fricken mountainous that it kills me that this factoid is not common knowledge.
From both personal experience and a lot of reading/research (see my Stuff I Love section), I know that our bodies have an awe-inspiring capacity to heal. Whole foods, exercise, stress management, and so on — they will promote lasting healing. While drugs save people with illnesses from a lot of suffering, I know that those drugs do not address the root problem and have many big-bummer side effects.
I would like to run around screaming bloody murder, but I try not to be a blatant freak. And since I have no medical training, I can’t blame anyone for patting me on the head when I preach. But I do have 15+ years of experience with a chronic illness, so can’t I warn people not to jump on this bandwagon to hell?
My older brother also has MS. We have no family history of MS — yes, that’s nuts. During a visit to his home, he lovingly served a bowl of sherbet to me after a great vegan dinner that he and his wife had made especially for me, and my eyes bugged out: dairy??? Don’t you know…don’t you care…don’t…d…” I was speechless. He might as well have served me a plate of venomous snakes, given the clear science on the effects of dairy (casein) on MS. He urged me to relax because “sherbet isn’t ice cream.” I felt ashamed by my knee-jerk reaction and my doubt that my brother would ever do anything knowingly to hurt me, so I gobbled up the sherbet. While we cleaned the dishes, I guiltily checked the ingredients on the sherbet box. First ingredient: milk. Big frowny face.
My brother is six years older than I am and was diagnosed with MS several years *after* I was diagnosed. His MS is in many ways less aggressive than mine, even though he is a true omnivore. I believe his MS success can be attributed at least in part to the fact that he exercises seven days a week, whereas I go to the gym three times a week. I feel like a turd for preaching to him. That said, I fear what my life would be if I hadn’t made radical changes to my diet, physical activity, and stress.
My mom was diagnosed as pre-diabetic several years ago. I was so excited to give her the great news! Studies are so clear that diet choices can save you from the ravages of diabetes. I begged her to read The China Study several years ago, which she said she did. Still, knowing all too well my obsession, she said carefully: “I am 75, and I am not going to change.” Another big frowny face. My mother! If I can’t convince my own mother, I need to reevaluate my messaging and keep trying. I have felt responsible for just my family. I had a 10+ year head start in this world of chronic illness. I should know better how to convince them.
It was my husband who changed my mindset, but I resisted, kicking and screaming. Back in 2010, he decided to become a vegetarian based on his concerns for animal welfare in industrial agriculture facilities. I told him that I didn’t want to be “that couple” that required dinner hosts to adapt their dinners to his weird needs. I genuinely worried that he would damage his health. Then I started to read, and read, and read, and read all the reasons that the standard American diet (SAD) is doing damage to animals, the earth, our bodies, our economy, and so on. Based on a mountain of scientific research with evidence of the health benefits, particularly for chronic illnesses, I leaped head first into vegan evangelism. I wondered why everyone else wasn’t leaping with me.
Recently, my 77-year old dad admitted that he too had been diagnosed as pre-diabetic. God! I felt surrounded and defeated. Chronic illness is no longer just in statistics. It is invading my family. I am the youngest and was the first in my family to be diagnosed with any illness. I should know how to help them to prevent their illnesses.
Only one (my older sister) is free of such a diagnosis. It literally kills me that I cannot convert them all so that we are safe from suffering, if that is ever possible.
So my heart burst with joy when my dad wrote me an email to let me know that he had cut out meat and dairy for the past month, while adding, “Why again do we not drink milk?” First, I was touched that he had launched into this big change without fully understanding the rationale. Second, we! Glee! Happy dance! My frown may start turning upside down! Somebody listened! And it’s my own dad!
I do not want to watch anyone I love suffer in pain or discomfort in his or her old age. I want us all to live well with a sound mind and body until we all die peacefully of “old age” in our sleep. Why should that be a crazy dream? Nowadays, it definitely seems crazy.
We all know that saying, “When the student is ready, the teacher will appear.” I was the tardiest student there ever could be, so I have got to accept that others will go at their own paces. I am trying very hard to focus on myself and not be “that person” who pesters and preaches, and who my friends and family barely tolerate. Given the statistics, though, I cannot be completely passive. I will aim to offer my loved ones an example of someone who is living well with MS. That’s all I can do.


You must be logged in to post a comment.